Faisal Shakeel,
Jamshaid Ali Khan ![]() ,
Muhammad Aamir,
Rabeea Shareef,
Nazia Shah
,
Muhammad Aamir,
Rabeea Shareef,
Nazia Shah
For correspondence:- Jamshaid Khan Email: jamshaidkhan@upesh.edu.pk Tel:+923009592943
Received: 19 May 2016 Accepted: 17 September 2016 Published: 31 October 2016
Citation: Shakeel F, Khan JA, Aamir M, Shareef R, Shah N. Identification of clinically significant drug-drug interactions in cardiac intensive care units of two tertiary care hospitals in Peshawar, Pakistan. Trop J Pharm Res 2016; 15(10):2289-2295 doi: 10.4314/tjpr.v15i10.31
© 2016 The authors.
This is an Open Access article that uses a funding model which does not charge readers or their institutions for access and distributed under the terms of the Creative Commons Attribution License (http://creativecommons.org/licenses/by/4.0) and the Budapest Open Access Initiative (http://www.budapestopenaccessinitiative.org/read), which permit unrestricted use, distribution, and reproduction in any medium, provided the original work is properly credited..
Purpose: To identify clinically significant potential drug-drug interactions in cardiac intensive care units of two tertiary care hospitals in Peshawar, Pakistan, and to compare the various potential drug-drug interactions related parameters between the government and private hospitals included in the study.
Methods: A prospective study was conducted in the cardiac intensive care units of the two hospitals, viz, Lady Reading Hospital Peshawar (LRH) and Northwest General Hospital and Research Center Peshawar (NWGH &RC), which are government and private hospitals, respectively. Samples of 260 and 250 patients from LRH and NWGH & RC, respectively, were evaluated. Patient medication charts were evaluated for potential drug-drug interactions and clinically significant potential drug-drug interactions using Micromedex DrugReax. The data were statistically analyzed.
Results: A high prevalence of potential drug-drug interactions was reported in both hospitals: 92 and 96.9 % in Northwest General Hospital and Research Center, and Lady Reading Hospital, respectively, of which half were clinically significant. A total of 19 interacting drug pairs contributed to the clinically significant potential drug-drug interactions. Independent sample t-test showed a significant difference in the potential drug-drug interactions of both hospitals. Furthermore, a significant relationship was found between the number of potential drug-drug interactions, on the one hand, and the number of prescribed drugs and age, on the other.
Conclusion: A high prevalence of potential drug-drug interactions, particularly clinically significant potential drug-drug interactions, calls for proper identification of these interactions and monitoring of patients to minimize adverse outcomes and improve patient therapy.
Introduction
Cardiovascular diseases are a prime cause of high mortality rates throughout the world. In 2012, World Health Organization (WHO) estimated that 17.5 million people died worldwide due to cardiovascular diseases. Most of these deaths occurred in low or middle income countries [1]. Risk factors include diseases like hypertension, hyperlipidemia, diabetes or other diseases which require multiple drug therapy, while behavioral risk factors include unhealthy diet, tobacco use, lack of physical activity and stress [2,3]. Furthermore, treatment for these diseases require multiple drug administration which when combined with factors like advanced age, co-morbidities and changes in hepatic and renal functions, increases the risk of potential drug-drug interactions (PDDIs) [4-6].
The presence of a potential drug-drug interaction (PDDIs) is highly probable in critical units like cardiac intensive care units (CCU), primarily due to the multiple drug therapy employed to combat the complex disease condition of the patient along with co-morbidities and age which further increases the risk of PDDIs [7,8]. However, not all the PDDIs are clinically significant and are not a predisposition of an adverse clinical event. Some PDDIs are employed to benefit the patient but these are very limited, for example the use of aspirin and clopidogrel in patients to prevent thromboembolism [9,10]. Apart for some rare instances, PDDIs are one of the leading causes of hospitalization [11,12].
Methods
This prospective cross sectional study was carried out in CCUs of two tertiary care hospitals of Peshawar, Lady Reading Hospital (LRH) and Northwest General Hospital and Research Center Peshawar (NWGH & RC). LRH is a government tertiary care hospital while NWGH is a private hospital. The duration of the study was one year and was approved by the ethical committees of both hospitals vide letter number 010 and NWGH/Research/01, respectively. Patient demographics, duration of stay, diagnosis, drugs administered, dose, frequency and duration of drugs prescribed were recorded from the medication chart of the patient. Names of the patients, their identification numbers and medical records were kept confidential. Good clinical practice (GCP) guidelines were followed under the declaration of Helsinki (1964) by the International Conference on Harmonization and Nuremburg Code [26]. Patients admitted to the CCU for at least 24 h and prescribed at least 2 drugs were included in the study.
Micromedex database DrugReax [13] was used to analyze the potential drug-drug interactions among prescribed drugs to the patients. This database provides information on the clinical effect, severity, documentation, onset and mechanism of the PDDIs. Severity may be major, moderate or minor; documentation may be excellent, good or fair; onset may be rapid, delayed or unknown; nature of PDDIs may be pharmacokinetic, pharmacodynamic or unknown; while mechanisms of PDDIs include absorption, distribution, metabolism, elimination, synergism, antagonism or unknown.
The severity and documentation of the PDDIs reported in Micromedex DrugReax was used to create a list of clinically significant PDDIs, on the basis of which the following PDDIs were considered as clinically significant:
• PDDIs having severity of major and of excellent or good documentation
• PDDIs having severity of moderate and of excellent or good documentation
Frequencies were used to summarize gender, number of prescribed drugs, diagnosis, duration of stay, frequency of PDDIs, interacting drug pairs and their severity, documentation, onset and clinical significance. Multiple linear regression was used to determine the relationship between number of prescribed drugs, duration of stay and the number of PDDIs. P values of ˂ 0.05 was considered statistically significant. Independent samples t test was performed to the compare the means of clinically significant PDDIs in both hospitals. All the analysis was performed using IBM SPSS Statistics for Windows, Version 20 (Armonk, NY: IBM Corp) [14].
Results
General characteristics
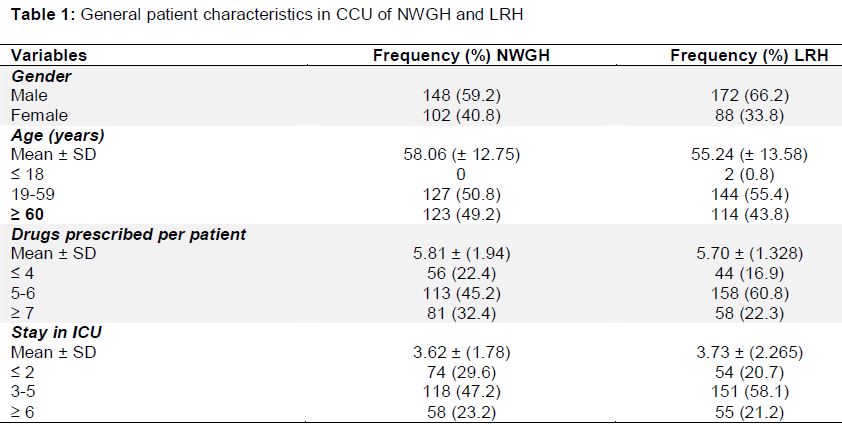
A total of 510 patient prescriptions were evaluated, of which 250 were from NWGH & RC, while 260 were from LRH, representing private and government sector respectively. The proportion of male patients as compared to female patients was higher in both the hospitals, 59.2 % in NWGH & RC while 66.2 % in LRH. The mean age of the patients was 58.06 ± 12.75 (range 19 - 88) and 55.24 ± 13.58 (range 12 - 95) in NWGH & RC and LRH, respectively. The median duration of stay was 3 days for both hospitals while the median number of drugs prescribed was higher in NWGH & RC (6 drugs per prescription) as compared to LRH (5 drugs per prescription). The general characteristics of the patients are displayed in .
Diagnosis
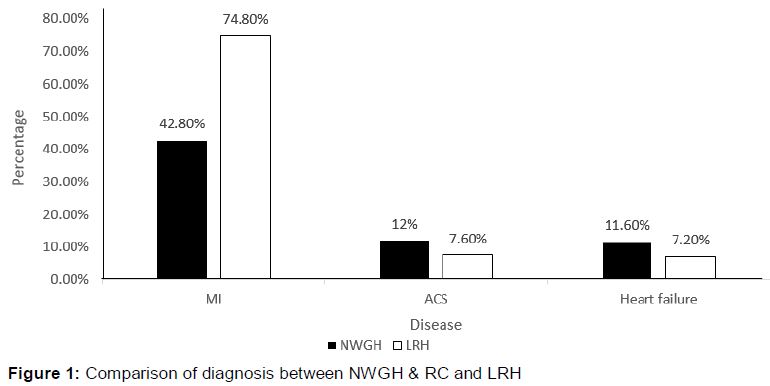
The most frequent diagnosis of patients admitted in both NWGH &RC and LRH was myocardial infarction (MI), while acute coronary syndrome (ACS) and heart failure were the other most frequent diagnosis of the patients. The comparison of the percentage of diagnosis in both hospitals is displayed in .
Prevalence of PDDIs and categories
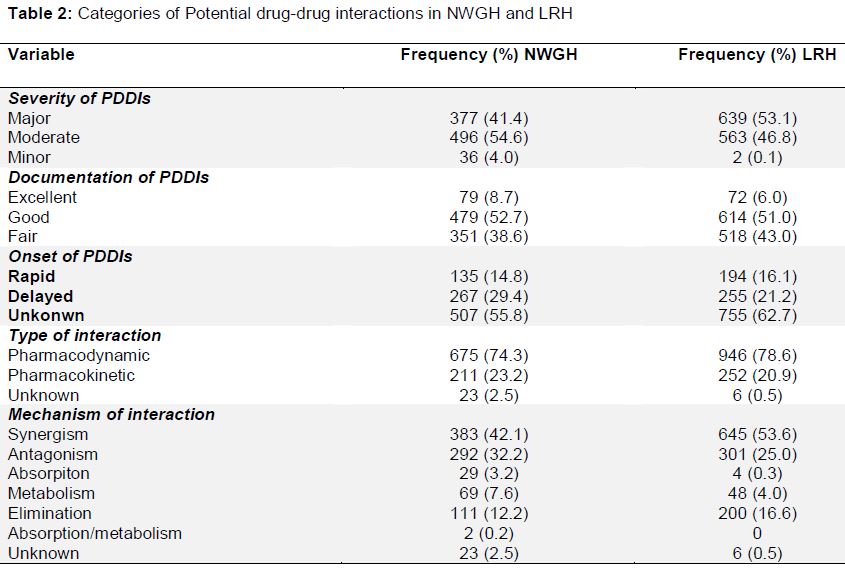
At least one potential drug-drug interaction (PDDI) was encountered in 92 and 96.9 % of the patients in NWGH &RC and LRH, respectively. A total of 105 interacting drug pairs contributed to the 909 PDDIs encountered in NWGH &RC while 76 interacting drug pairs contributed to the 1204 PDDIs encountered in LRH. The severity, documentation, onset, nature and mechanism of the PDDIs encountered in both hospitals are displayed in .
Clinically significant PDDIs
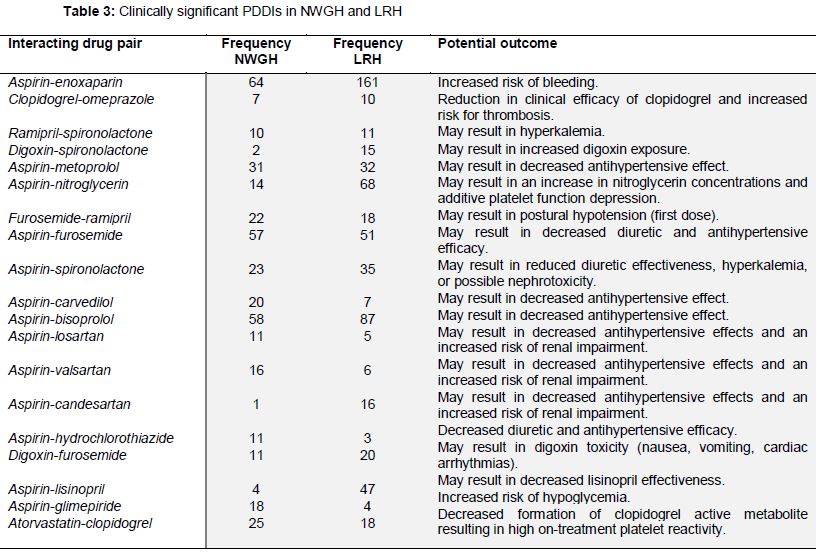
Clinically significant PDDIs were identified using the predetermined criteria. Using this criteria along with the frequency of PDDIs, a list of 19 interacting drug pairs was prepared from both the hospitals which were considered to be significant clinically, because of the associated high risk and occurrence in the cardiac critical care unit. The list of clinically significant PDDIs from both hospitals along with their frequencies and potential outcome is displayed as . These PDDIs contributed to 44.6 and 51 % of the total PDDIs encountered in NWGH & RC and LRH respectively. Furthermore, it was observed that 3.63 and 4.63 PDDIs were present per patient in NWGH & RC and LRH respectively while 2.07 and 2.54 clinically significant PDDIs were present per patient in the hospitals respectively.
Independent sample t-test
An independent sample t-test was performed to compare the means of clinically significant PDDIs between NWGH and LRH. The t-test showed a significant difference (t = 3.435, p = 0.001) in the number of clinically significant PDDIs between NWGH and LRH.
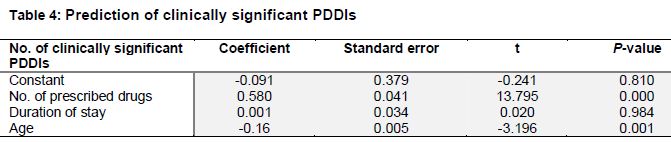
Prediction of clinically significant PDDIs
Multiple linear regression model was fitted to predict the number of clinically significant PDDIs based on number of prescribed drugs, duration of stay and age. The effect of number of prescribed drugs on number of clinically significant PDDIs, controlling for the effect of duration of stay and age, was found to be significant. (t = 13.795, p < 0.0001). The effect of age on number of clinically significant PDDIs, controlling for the effect of duration of stay and number of prescribed drugs, was also found to be significant. (t = -3.196, p = 0.001). The effect of duration of stay on number of clinically significant PDDIs, controlling for the effect of number of prescribed drugs and age, was found to be insignificant (t = 0.020, p = 0.984) ().
Discussion
This study reported a high prevalence of PDDIs which corresponds to other studies reporting a similar higher prevalence in cardiology. University of Pittsburg conducted a study in cardiac and cardiothoracic ICU patients, found 87.7 % patients having at least a single PDDI [15]. Cross sectional studies conducted in Pakistan also reported a prevalence of 91.1 and 77.5 % cardiology patients having a PDDI [4,16]. It was also reported that 72.5 % of ICU patients had PDDIs in the ICU of a Brazilian hospital [17]. While another Brazilian study reported 87.2 % patients in cardiology encountered a PDDI [18].
A Brazilian study evaluated 1785 prescriptions and recorded similar trends as seen in this study with the severity of most PDDIs being moderate (78.6 %), documentation of most PDDIs was good (29.5 %) and most (42.5 %) were pharmacodynamics in nature [19] Another study reported PDDIs of moderate severity to be the most common (62.5 %) [20]. In 203 patients, 75.03 % of PDDIs were in Category C which corresponds to moderate severity [21]. A record of 1124 patients were evaluated for PDDIs at 24 h and 120 h after admission to the hospital. The severity of most interactions was moderate in both the time frames (50.1 and 51.4 %), most of the interactions were good documentation (63.9 and 59.1 %) and most of were of pharmacodynamic in nature at 120 h (45.2 %) [22]. To our knowledge no previous study has focused on the clinically significant interaction in cardiac intensive care units. Our study shows that 3.63 and 4.63 PDDIs were present per patient in NWGH & RC and LRH respectively while 2.07 and 2.54 clinically significant PDDIs were present per patient in the hospitals respectively. This is of great concern because more than half of the PDDIs encountered were clinically significant and can have a significant impact on the advanced disease condition of the patient.
A significant association was found between clinically significant PDDIs and number of prescribed drugs and age of the patient. This association was similar to that of reported in other studies [4,18,23-25]. A Nepalese study reported a significant linear association between length of stay and occurrence of PDDIs [20]. Another study conducted in cardiology department of Pakistan also reported a significant association between PDDIs and prescribed drugs and age [4].
Proper PDDIs identification and management system are lacking in these hospitals which contribute to this high prevalence of PDDIs. Pharmacists should update themselves regarding the knowledge of clinically significant PDDIs and timely interventions implemented.
Limitations of the study
Monitoring of the adverse outcomes due to the PDDIs and lack of interventions were some of the limitations of this study. This study identified clinically significant PDDIs on the basis of literature and drug interaction database, while clinical studies can be conducted in the future to monitor the actual clinically notable adverse outcomes of these PDDIs and their effect on the patient disease.
Conclusion
This study identified not only a high prevalence of PDDIs but also clinically significant PDDIs which have greater potential for significant changes in patients’ condition. Also notable was the significant difference in PDDIs between the private and government hospital, which demands for the implementation of proper drug interaction monitoring systems across all hospitals to minimize this health care hazard.
Declarations
Acknowledgement
References
Archives


News Updates